
 Yesterday I attended ‘Parents’ Voices and their Experiences of Services’ at Friends Meeting House in Manchester. It was an opportunity to examine priorities for system, policy and practice change, drawing upon findings from research and was a very valuable day for reflective practice. The event began with a short introduction by Safeguarding Survivor who chaired the conference with great confidence and professionalism. I know she was nervous but you couldn't tell and she did a brilliant job. If you aren't aware of her story, I recommend you read her blog. It offers great insight into the child protection system from a parents’ perspective and provides excellent advice for others whose children have been identified as ‘at risk’. Her work has been praised for its balance and value by Sir James Munby and you will soon be able to read more of her case after the court granted Louise Tickle (a freelance journalist) permission to publish details in a broadsheet newspaper. You can read the judgement at Family Law.  Siobhann and three mothers from The Mothers Apart project (Women Centre) Kirklees spoke about their book In Our Hearts. It presents open and honest accounts of initial separation, court proceedings, relationships with services, of mothers who have been able to have children returned to their care or contact increased, mothers who have no current contact at all and those for whom contact remains limited. It offers itself up as an aid and guide to learning for parents, families and professionals working in pursuit of child protection. As a result of co-production learning Mothers Apart have developed women centred working that recognises people as assets. Whilst every woman is different they have found that there are a number of common themes and, consequently, much of their work is about power. Sean Haresnape (Principal Social Work Advisor) from Family Rights Group outlined a Parents Charter being developed in collaboration with parents and professionals, that sets out expectations of how services should engage with parents, whose children are subject to statutory interventions; and we heard from Declan, a father and care leaver who had his daughter placed with him following care proceedings. Prof. Karen Broadhurst (Lancaster University) and Claire Mason (ISW & Lancaster University) presented preliminary findings from their 2 year study of birth mothers, their partners and children, within recurrent care proceedings under s.31 of the Children Act in England. The project hopes to confirm the national scale and pattern of recurrent proceedings together with the characteristics and service histories of parents caught up in this cycle. Statistical methods have been used to quantify recurrence and examine the relationship between recurrence and key explanatory variables. This has been complemented by qualitative components that include in-depth interview work with birth mothers in five local authority areas and in-depth profiling of a subset of randomly selected case files. 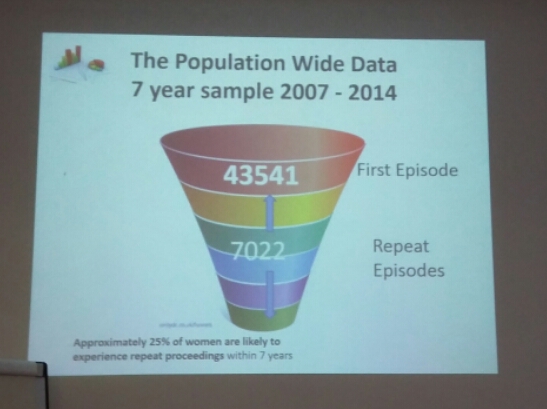 Through data mining they have found that 25% of women who have been through care proceedings will return within 7 years. Teenage motherhood is associated with a significant number of repeat care proceedings and Prof. Broadhurst questions whether the family court is the most appropriate setting for dealing with teenage parents. 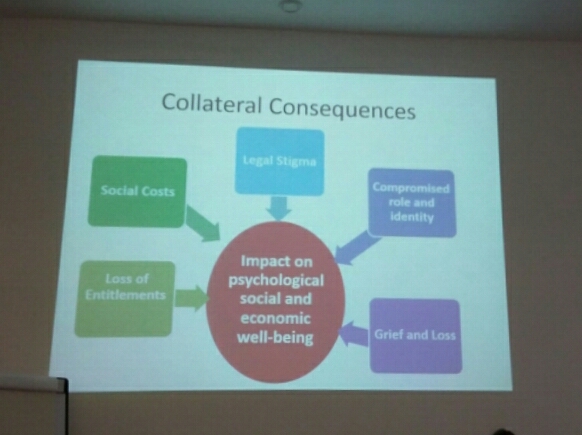 Another facet of their research looks at the collateral consequences of care proceedings and asks who, once a court case has concluded, is there to support parents with the psychological, social and economic consequences of losing a child. Whilst the child and adopters/foster carers remain supported for a time by Social Workers and other services, there are no statutory support available to parents. This short-sighted approach demonstrates a lack of understanding of the collateral consequences and their cumulative impact which can drive women in to unhealthy relationships and successive pregnancies. In subsequent cases Local Authorities and Courts have been found to act more swiftly and are more likely to remove closer to birth, with adoption being the most likely outcome, compounding the cycle.
Similar concerns were raised last week by Sir James Munby when I attended the annual Family Justice Council debate in London. He said that it was “not fair on subsequent children that post adoption support isn't provided to birth parents” and “there is some substance to the question whether resources are adequately balanced between support for adoption and support for families”. Finally, Prof. Kate Morris (Sheffield University) outlined the empirical research she and Prof. Brid Featherstone (University of Huddersfield) are conducting as part of Your Family Your Voice – an alliance of families and practitioners working to transform the system. Their work, looking at family experiences of multiple service use, highlights the profound difficulty families often find navigating their way through services. At the end of the presentations we were asked to reflect upon what we had heard and identify what changes could be made to make the system a more humane one and minimise trauma for parents, children, their families – and also for practitioners. I invite you to do the same and participate in the research here.
1 Comment
 As part of my research I have been looking at the construction of parenting and, specifically, mothering. How expectations of the parenting role has changed over time and how this has shaped and been shaped by government policy and legislation. I'm going to try and blog about pieces that I think will be particularly interesting to Social Workers, as I know quite a few of you follow my page, but I'll try not to bombard you too much with academic content.
Today I read The Social Work Assessment of Parenting: An Exploration by Johanna Woodcock. Although it was published in the British Journal of Social Work over a decade ago (2003) I believe her findings are still relevant today and would be a good read for any practitioner wanting to reflect upon their own construction of parenting and practice. Woodcock’s paper draws on a qualitative study of Social Workers conceptualisations of parenting and the relationship this construction has with practice. Within her exploratory study, Social Workers were asked to describe and give their opinions on the parenting that occurred within a case that they brought forward. Analysis of the data she obtained revealed four types of expectations that underlay judgements of parenting deemed both ‘good enough’ and ‘not good enough’. 1. The expectation to prevent harm. Woodcock found that Social Workers were influenced by legal or quasi legal constructions of parenting. Their overriding concern was the capacity of the parent to prevent harm and relied upon the presence or absence of evidence of ‘physical abuse’ ‘emotional abuse’, ‘sexual abuse’ or neglect in making this judgement. 2. The expectation to know and be able to meet appropriate developmental levels. Woodcock found that Social Workers attributed a parent’s failure to protect their child from harm to their limited understanding of their child’s stages of development. Woodcock highlighted the narrative from one case where a parent and social worker were unable to agree on the level of appropriate supervision. A second area of Social Worker concern manifested when a delay in growth and development was deemed to be the result of poor parenting. 3. The expectation to provide routinised and consistent physical care. Parents were expected to appreciate the importance of routines and demonstrate their capacity to carry them out Woodcock found that routines were a key element of Social Work discourse. ‘Not meeting the child’s needs’ invariably referred to a lack of routine and consistency and that the child’s emotional needs for a sense of safety and security were not being met. 4. The expectation to be emotionally available and sensitive. For some Social Workers it was insufficient for a parent to simply love a child. They needed to have more insight into the emotional reasons for a child’s behaviour, which took them beyond physical care and to demonstrate a level of affect and interest in the parent-child interaction. Woodcock also looked at the Social Workers’ ‘psychological appreciation’ of the parent. She found that one way in which social workers made sense of problem parenting involved whether the parent was psychologically ‘damaged’ or ‘disturbed’ through abuse, or a lack of consistency or emotional warmth in their own childhood. Alternatively, early experiences were seen to provide modelling for future parenting and the absence of a positive role model accounted for their lack of ‘knowledge'. Importantly, Woodcock noted that these explanations draw on two implicit competing theoretical orientations: psychoanalysis and social learning theory; and despite being assimilated into assessment this evidence base was not evident in intervention or treatment. Conversely, Social Workers relied on exhorting parents to change or ‘getting them’ to take responsibility. She found little evidence of attempts through intervention to address these deeply ingrained psychological needs, either through direct social work or referral to psychological services. When psychologists were called upon it was to contribute an opinion with regard to the parent’s capacity to change rather than to help facilitate that change. Woodcock asserted that it was this incoherence between the intervention strategy and the social workers construction of parenting which inevitably led to resistance. Somewhat ironically, it is also resistance and an ‘inability to work with agencies’ that compounds an assessment of poor parenting. The main concern for practitioners should be Woodcock’s identification of a ‘surface static’ notion of parenting. A surface response means that the psychological factors underlying parenting problems remain unresolved. By relying on exhortation to change, rather than responses informed by psychological observations, Social Workers create an environment that is unconducive to change and thus perceptions of parent ‘resistance’ more likely. An explanation offered by Woodcock for the presence of a ‘surface-static model’ is the fact Social Workers are increasingly directed to their legal responsibilities to ensure the protection of the child from harm, rather than on problems that beset the parent. This professional quandary has, in my opinion, only worsened in the intervening decade and is something that government needs to address if outcomes are to improve. Social Workers need to reject the current political rhetoric surrounding parenting which places responsibility for child outcomes with parents, whilst underplaying socio-economic factors. On a practice level, Social Workers can consider what constructs they being to an assessment and whether their work reinforces a static notion of parenting. Try and incorporate these questions into your reflective practice: Am I focussing solely on assessment and parental behaviour, or am I actively seeking to enhance parental capacity through improvements in the problems that beset the parent. I imagine this would be an interesting discussion in supervision.  Recently I’ve been posting about attachment after the National Institute for Health and Care Excellence (NICE) argued more should be done by health and social care providers to train key workers in assessing attachment difficulties and parenting quality. Firstly I outlined the origins of attachment theory and then went on to detail some of the current debates. Over the years I have read many assessments of children and their families in which workers have assessed attachment as being ‘good’ as the child had been seen “happy and smiling”. In the serious case review of Peter Connelly it is noted that the social worker reported “he had a good attachment to his mother, smiles and is happy”. Two months later a second social worker reported “a good relationship between the child and his mother” despite him head-butting the floor and his mother several times. These behaviours in and of themselves are not indications of attachment. In instances of abuse, smiling may be a learned defence mechanism which they have developed to put their carer at ease thereby making them safer. It is, therefore, important that Social Workers develop skills to correctly assess attachment and its impact upon a child’s internal working model. I have already touched upon Mary Ainsworth’s Strange Situation in my previous posts but will go into a little more detail here. NICE recommended in their draft guidance that practitioners should consider the use of the ‘Strange Situation Procedure’ for children aged 1-2 years, and a modified version for 2-4 year-olds. The procedure is used in a controlled setting and practitioners observe the child’s response to two brief separations from, and reunion with, the parent. The child’s responses are then categorised as fitting one of three patterns of behavioural organisation:
Take a look at the following YouTube video by The New York Attachment Consortium to see how these behaviours manifest in practice. Children’s’ responses in this situation are considered to reflect the history of interactions the child has experienced in the home. However, research has found that on occasion and child’s Strange-situation behaviour does not fit well into the criteria of any of the given classifications as described by Ainsworth. It is therefore, important that practitioners do not ‘force’ a child into the ‘best fitting’ attachment classification. It may, in fact, be that a number of different, coherent and distinct responses are possible. Disorganised or disorientated behaviour is one further classification that has been identified and is seen by Social Workers in cases of abuse. These behaviours can be identified when a child finds themselves in anxiety-provoking situations into which an abusive caregiver enters. As the child does not know what to do they experience “fear without solution” and practitioners will observe simultaneous displays of contradictory behaviour patterns. NB. when using the Strange Situation procedure it is important Social Workers are mindful of the fact that behaviour could be a function or neurological or other difficulties experienced by the infant as an individual, having little to do with relational issues between parent and child. Recent research has moved away from observations of behavioural interactions between infants and parents, like the Strange Situation, and Social Workers should also be concerned with how attachment experiences become organised in memory into “models” of relationship expectations. This shift reflects a recognition of the important role that internal working models play throughout life. They form the “schemas” that predispose a child to perceive social relationships in terms of past experiences. Any assessment should also, therefore, be interested in understanding how children form and organise internal working models of attachment experiences.  Social Workers have for many years relied on play as the primary medium of communication as it provides a compensating medium for limitations in children’s verbal abilities. Additionally, the expression of emotionally charged adverse experiences often makes direct verbal communication more difficult for children, and Social Workers are sensitive to this.
Using dolls, the Story Stem Assessment Profile asks children to respond to a set of narrative story stems where they are given the beginning of a ‘story’ highlighting everyday scenarios with an inherent dilemma. Children are then asked to ‘show and tell” me what happens next?’ This allows some assessment of the child’s expectations and perceptions of family roles, attachments and relationships, without asking the child direct questions about their family which might cause them conflict or anxiety. If you are going to employ this technique I would recommend that you use dolls that are ‘neutral’ like these from Melissa and Doug. Using figures from known television programmes could encourage the child to script the story in a way that is congruent with the toys ‘character’ rather than their own internal working model. Clinical training in this technique is available through the Anna Freud Centre in London. I hope you have found my posts helpful and interesting. They contain just a fraction of the information provided through professional training and I would recommend practitioners incorporate this into their continuing professional development plan. I will add a further post soon about assessing attachment in older children. Please follow me on facebook or twitter to catch it.  Last week I started a 6 week course with the University of Edinburgh called The Clinical Psychology of Children and Young People. Child psychology is an area that particularly interests me and I'll post some of my own interpretations of how the material can be used in social work practice. I have studied it extensively in the past; however, I believe that as Social Workers we should continually refresh and build upon the knowledge that forms a basis for our practice. Like renewing a first aid certificate. I hope you find these posts interesting and helpful. This week we looked a child and adolescent development, factors that influence development, and models of developmental psychopathology. An understanding of children’s development helps us to interpret children’s well-being and mental health, and taking a developmental approach is important as it helps us to spot and interpret a number of different patterns and behaviours. Furthermore, looking at developmental outcomes (milestones) allows us to see when development is atypical and helps us to identify ways in which the child may need supporting.  Children are qualitatively different from adults, they are not born as mini adults, and they are not born as empty vessels. They are complex in their development: some development occurs slowly and over time; other times development occurs rapidly such as in infancy and adolescence. To help, we can break it down into the following phases of development:
There are also different aspects of development:
Of course, the child develops as a whole and the different aspects of development do not occur in isolation. They all interact with one another. To understand this we look at patterns of development. Development isn't always progressive. There are various patterns of continuous change. Sometimes development can be very rapid and sometimes change is slow and gradual. At 18 months children start to engage in pretend play. Pretend play starts to decline during middle childhood as other forms of play become more prominent. This pattern of continuous development is often known as an inverted U function; where you can see that development increases and then declines. You can also have U shaped continuous change where you see an apparent decline that actually leads to an improvement in development. Often this is true of cognitive development where a child’s behaviour may look like it is becoming more difficult but actually, cognitively, they are re-evaluating how to perform the task and then their performance improves. Another pattern of development is stage changes. This is where you have changes in ability which seem to take quite a dramatic shift. A classic theory of stage changes is Piaget’s theory of development. He outlined four stages of cognitive development:
Piaget argued that each of these stages is typified by a new range of cognitive abilities or operations that allow children to cognitively perform at a different level. There are many influences on development. Firstly, biological influences like genetics and the brain. Genetics have a probabilistic relationship with development. They do not always determine or cause different developmental outcomes but they influence it through interacting with other genes and other things in our environments. An example of where genetics do have a direct link with development is in Down Syndrome. It’s a chromosomal abnormality that lead to a particular set of features and characteristics. Most genetic contributions are, however, probabilistic and they are seen as a risk or protective factors rather than direct causes. Twin research studies have been helpful in assessing the relative role of genes versus environment. As a result some mental health conditions and difficulties have been found to have a genetic component to them. For example, schizophrenia, ADHD, Autism, developmental dyslexia. However, genes aren't the whole story they are just a part of it. The Human Genome Project has helped to identify which genes or constellation of genes influence particular developmental and mental health outcomes. For example, we now know particular genes are involved with autism. We also know that some genes and combinations of genes act as protective factors as well. Brain development is also a significant biological influence. We know that there are important growth spurts which occur in the brain, firstly in infancy, and then later in adolescence. In the first two years of life we know that the brain grows enormously; but even more important are all the connections that are made in the brain that are related to the experiences the child has both physically, socially and emotionally. The more experiences a child has the more connections are maintained. If those experiences don’t occur or are reduced then the synaptic connections are pruned. This means that early brain development in infancy is very much a product of the environment the child is in; but in turn that brain development itself offers developmental opportunities for the child. The next major changes in brain development occur in adolescence which coincide with puberty. I’ll write a separate post on this later. Biological influences are really important but the environments within which children live and the people they live with are crucial to their development. We refer to these as social and environmental factors. Not only do the people a child lives with influence the food they eat (whether they have enough), the house and community they live in but also the people around them give them opportunities to learn and improve their understanding of the world and themselves. Also the people around them help them to form relationships and emotional bonds with others which can last in the long term. Social workers can use a tool (based on Bronfenbrenner’s Ecological systems theory) to assess a child’s social and environmental factors. A child can complete a task with concentric circles with them in the middle; identifying who they think are important to them. Most importantly you should ask the child why they feel they are important. 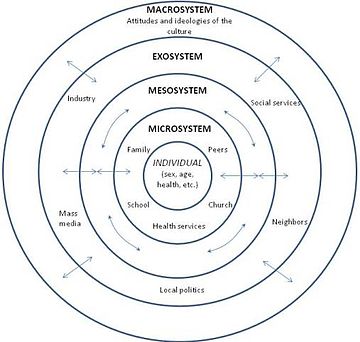 The third influencing factor on development is the interactions between biological, psychological and social influences. Most of a child’s development is influenced by both biological and social factors and how they interact. This area is often called the nature / nurture debate. For example, in early infancy, experiencing a loving, caring relationship with someone is crucial to the development of attachments. If this area is of particular interest you might like my posts on Psychology and Mental Health: Beyond Nurture and Nurture. Finally, we looked at models of developmental psychopathology and it’s influences on mental health and well-being.  Developmental psychopathology focuses on normal and abnormal development and also adaptive and maladaptive processes. It shows us that there are a range of developmental trajectories that a child can take. Compas and colleagues undertook a review of adolescent development and highlighted that there isn’t just one developmental pathway or trajectory. They identified five:
This model is important as it highlights that adolescent development doesn’t just have one pathway. There are a range of different pathways that young people can find themselves on depending on a range of different factors and influences. 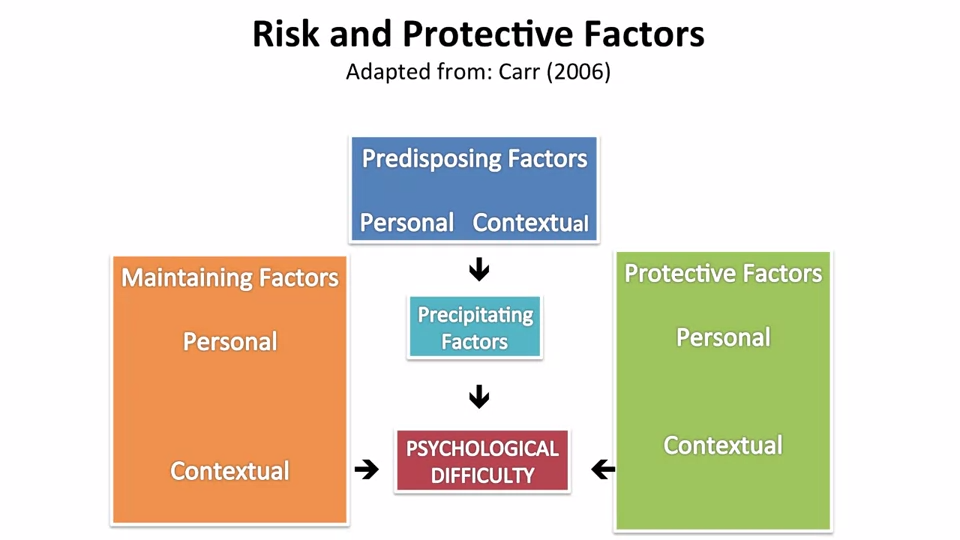 Social Workers work with children and use skills based upon child development in their everyday practice. We observe children and learn something about how they’re developing and their well-being from our observations of them. We speak to children and learn about their development directly from them. We sometimes use little tasks and drawings and even short questionnaires and scales. If you'd like to find examples of scales and questionnaires that might be helpful in your practice please take a look at the tools section of this website.
Next week I'll be covering the topic of resilience. Please follow me on facebook or twitter so you don't miss it!  I've written a couple of posts recently about Protecting Young Children Online and Protecting Big Kids Online. I was thrilled at how many times they were viewed and shared (Thank you!) and I hope they have helped you to feel more confident in safeguarding your children in the digital age. Since I last posted I've found the new Fire HD Kids Edition. It has some great easy-to-use parental controls where you're able to manage usage limits, content access and educational goals, plus there's a 2 year worry free guarantee! It looks fab! Children’s apps and websites were in the news on privacy grounds earlier this week, after the UK’s Information Commissioner’s Office (ICO) announced a review of how these services collect data on their young users. It will form part of an international project, coordinated by the Global Privacy Enforcement Network, and will look at 50 websites and apps, particularly what information they collect from children, how that is explained, and what parental permission is sought. The websites and apps will include those specifically targeted at children, as well as those frequently used by them. So how can parents decide which sites, apps and games are appropriate? Today I was emailed about the NSPCC's updated Net Aware guide which helps parents to understand what their children are doing online and hopefully maintain open channels of communication. It's a huge database providing information on sites, apps and games. It tells you what it is, why kids like it and provides an age rating to help parents judge whether it's appropriate for their child. After having a look through the site I realised that I probably haven't heard of half of them before.  Research by the NSPCC earlier this year found that many parents have gaps in their online knowledge and don't talk about the right issues with their children. For example, Tinder, Facebook Messenger, Yik Yak and Snapchat were all rated as risky by children, with the main worry being talking to strangers. However, for the same sites the majority of parents did not recognise that the sites could enable adults to contact children.
Although eight out of ten parents told the NSPCC that they knew what to say to their child to keep them safe online, only 28% had actually mentioned privacy settings to them and just 20% discussed location settings. One of the best ways of safeguarding your child online is to maintain open channels of communication. Here are my top tips:
Take a look at the NSPCC guide and let me know what you think.  For the last three weeks I've been posting about a course I've been taking called Psychology and Mental Health: Beyond Nature and Nurture. This week we focused on the role of psychological mechanisms in the development of mental health problems and the maintenance of well-being. The sources we were presented with suggest that a psychological perspective adds a vital additional element to the ‘nature-nurture’ debate, because it is through these psychological mechanisms that we interpret and respond to the world.  Our course leader Peter Kinderman, Professor of Clinical Psychology at the University of Liverpool, argues that our mental health is essentially a psychological issue, and that biological, social, and circumstantial factors affect our mental health and well-being by disrupting or disturbing psychological processes. The way in which we make sense of the world, the way in which we understand ourselves, who we are as people, the way we make sense of other people, the way that we react socially, how we think about the future, and how we think about the world in general, this sense making, this framework of understanding of the world is fundamentally important in determining our mental health and well-being. To get us started we are provided with a copy of Peter Kinderman’s, A Psychological Model of Mental Disorder. This article discusses the relationship between biological, social, and psychological factors in the causation and treatment of mental disorder. He suggests that a comprehensive psychological model of mental disorder can offer a coherent, theoretically powerful alternative to reductionist biological accounts while also incorporating the results of biological research. We are told that Peter was able to test out some of these ideas in a research study that he conducted with the help of the BBC; testing out the idea of whether a combination of different factors could predict the level of mental health difficulties and well-being that a person was experiencing. They were interested in whether biological factors, which were measured by looking at the experience of mental health problems in a person's family of origin, in their parents and in their siblings, could predict mental health problems, which would then have a variety of psychological and social consequences. Or whether, on the other hand, life events like trauma in early childhood or experiencing a range of negative life events in the last six months would predict people's mental health problems. Or as they hypothesised, whether psychological factors - rumination, where people would go over and over things in their minds, or self blame, where people would blame themselves for the difficulties they were experiencing - would explain more of a person's mental health problems. 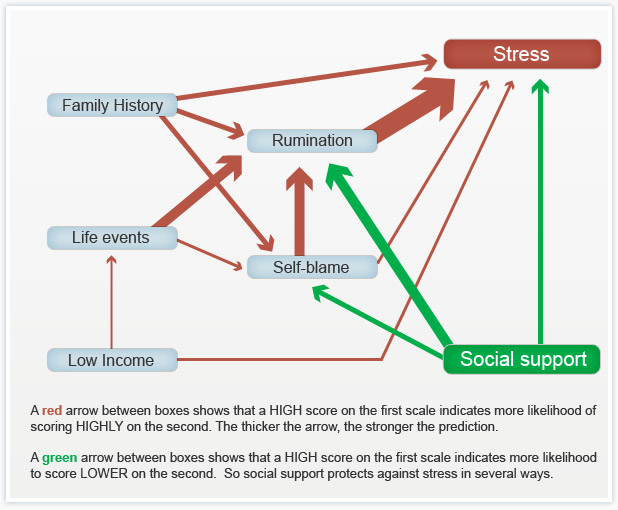 When they looked at the results, it seemed that social factors were very influential in predicting people's mental health problems, with biological factors playing a part, but a less important part. But importantly, both social and biological factors were mediated by the psychological factors. So, they asserted, rumination and self blame seem to be the gateways towards mental health problems.
You can see the paper itself and also a brief magazine article (Rumination: The danger of dwelling) hosted by the BBC on their website. Peter says that this way of thinking about mental health has some quite profound consequences. If you realise the way in which a person thinks about the world, the way in which a person responds to events in their lives, makes a difference to their mental health, to their well being, to anxiety and depression, it does change the way in which we should approach mental health problems. It brings it back to the idea that how we think about the world matters. Because it changes the way in which we feel and behave. This gives us some different opportunities for how to help people who've got emotional difficulties. But it's also important for people who themselves are suffering, because rather than blaming them for their difficulties, it means that there are things that they can do themselves to get out of the problems that they find themselves in. It gives people a sense of agency and control over their own mental health. Finally we were invited to take part in some of Peter’s current research: Causal and mediating factors in mental health and wellbeing. A follow up study to the research that has formed the basis of this week’s part of the course. At the end of the course we are asked if we believe adding psychological processes to the mix add anything useful to our understanding of the ‘nature-nurture’ debate? Do we think these kinds of factors are important in determining our mental health and well-being? Do we think an understanding of psychological processes mean that we can offer more useful ways of helping people - perhaps through therapy? What do you think? If rumination is posing a difficulty for you or a client there are a couple of things you could try.
 I read in the Guardian today that Downing Street have announced Iain Duncan Smith will remain Work and Pensions Minister following the Conservatives electoral win last week. They reported that he will “continue with his task of “making work pay and reforming welfare” as the government implements the universal credit reforms and imposes £12bn in cuts on the welfare budget”. This will be in addition to the £30bn that the Institute of Fiscal Studies say the Tories will also need to find in real-terms cuts from ‘unprotected’ departments, including social care and defence. The news of a Tory win last Thursday didn’t go down well with some. There were large demonstrations in London over the weekend; although it was only the violent clashes with riot police outside Downing Street that seem to have made the headlines. However, the arrests don’t seem to have deterred them; and the anti-austerity group behind the protest are planning another demonstration outside the Bank of England next month. Like many, I am genuinely worried about the proposed cuts and what that means for social work. I posted last week that Peter Kinderman, Professor of Clinical Psychology & Head of the Institute of Psychology, Health & Society at the University of Liverpool, has said that one of the best predictors of mental health disorders by far, whether it’s depression, suicidality, psychosis, are all life events. The strongest predictor all by itself is poverty. Not because poverty by itself causes depression, but because it is a predictor of all the other things that are causal. So poverty has been described as the causes of the causes. And those other causes are a whole raft of things – childhood neglect, childhood abuse, loneliness, and problematic parenting, which is usually inter-generational. It’s not about bad parents, it’s about who themselves haven’t perhaps had the sort of childhood that predisposed them to good enough parenting. And so the cycle continues… There are currently 3.5 million children living in poverty in the UK. That’s almost a third of all children. 1.6 million of these children live in severe poverty. But what the Conservatives don’t want you to know is that 63% of children living in poverty are in a family where someone works. This is why welfare, preventative services, family support and intervention are so vital. We need to break the cycle by providing welfare that brings children out of poverty. Services need to be funded and available to support the most vulnerable and improve parenting so that children can be safeguarded in the care of their family. However, services that were once available have been decimated through cuts over the course of the last parliament and they look set to get worse by 2020. But welfare isn’t just about being a decent human being; it also makes economic sense. In the mid-'90s, the Centers for Disease Control and Prevention discovered an exposure that dramatically increased the risk for seven out of ten of the leading causes of death in the United States. In high doses, it affects brain development, the immune system, hormonal systems, and even our DNA. People that are exposed in very high doses have triple the lifetime risk of heart disease and lung cancer and a 20-year difference in life expectancy. It’s not about eating GM foods. It's childhood trauma: things like abuse or neglect, or growing up with a parent who struggles with mental illness or substance dependence; things that we know, according to Peter Kinderman, are strongly linked to poverty. Take a look at this 2014 TED talk by Nadine Burke Harris. The Adverse Childhood Experiences study found that there was a dose-response relationship between ACEs and health outcomes: the higher your ACE score, the worse your health outcomes. For a person with an ACE score of four or more, their relative risk of chronic obstructive pulmonary disease was two and a half times that of someone with an ACE score of zero. For hepatitis, it was also two and a half times. For depression, it was four and a half times. For suicidality, it was 12 times. A person with an ACE score of seven or more had triple the lifetime risk of lung cancer and three and a half times the risk of ischemic heart disease, the number one killer in the United States of America.  Now, you might be thinking – this is interesting but it’s about a study conducted in the United States. Can we rely on the findings to support welfare as a public health initiative in the UK? Well…. In 2014 Mark Bellis and colleagues published a retrospective study to determine the impact of adverse childhood experiences on adult health behaviours and health outcomes in a UK population. They also found that increasing ACEs were strongly related to adverse behavioural, health and social outcomes. Compared to those with 0 ACEs those with 4+ ACEs had a greater risk of poor educational and employment outcomes; low mental wellbeing and life satisfaction; recent violence involvement; incarceration; recent inpatient hospital care and chronic health conditions; and early unplanned pregnancy. All of this suggests a cyclic effect where those with higher ACE counts have higher risks of exposing their own children to ACEs. There are more studies here, here, and here. It’s clear that these childhood experiences place a burden on a UK population’s health, NHS and judicial system; and there is a strong case for the government to invest in effective interventions to prevent them. That’s why the World Health Organization and global health partners are promoting research into the extent and impact of them around the world. So, why is it that during this time of growing evidential support for preventative work, is the government promoting a false economy through welfare cuts and dismantling the welfare system??? In 2007 Lynne Wrennall identified failures in the UK’s work with vulnerable children. She believes that the morale of a “great many caring, compassionate, highly competent, and creative social workers” would be “vastly improved if their primary function was again focused on assisting, rather than dismantling, families, upon working creatively toward this end with the resources and the legislative and managerial support to do so”. However, she also acknowledges that sometimes “an out-of-home placement is unavoidable”, and that in those instances “a programme leading towards re-unification and rehabilitation must be implemented”. She advocates for a “European model” that “strongly favours an educative role for social workers and a primary task of maintaining family unity, utilising and coordinating services toward this end and focusing on `educating’ the parents and family in social norms and values”. But for this to happen the conservative government would first need to reframe the way it thinks about the most vulnerable people in our society and invest in their future wellbeing and health. Local Authorities would need greater funding to hire more social workers so that caseloads are at a manageable level where they have the time to undertake intensive direct work with families again. They would need to fund preventative and outreach services that can directly tackle problems before children become at risk of significant harm. Instead, proposals have been tabled to jail social workers who fail to prevent neglect, despite the necessary infrastructure to properly address it; and the shock result of a Conservative majority victory signals deeper, faster cuts than ever before. Communitycare has urged Social Workers to channel whatever they are feeling about the election result into something that isn’t apathy, because the profession looks set to be needed like never before and I have to agree. P.S. Please follow me on facebook and/or twitter to see posts as they're added to my site
 For the last two weeks I've been posting about a course I've been taking called Psychology and Mental Health: Beyond Nature and Nurture. So far I've found it really interesting and it has challenged me to reflect on my practice and past cases.
Last week, we discussed the role of biological processes and mechanisms. We were urged to consider how our emotions, thoughts and behaviours are related to neurotransmitter and other biological mechanisms; and to appreciate how this shapes service provisions. This week we were taught about the role of psychological mechanisms in the development of mental health problems and the maintenance of well-being. The material we were presented with highlighted a vital element to the ‘nature-nurture’ debate, asserting that it is through these psychological mechanisms that we interpret and respond to the world. Many psychologists and psychiatrists believe that it's by looking at the nurture side of the equation, by looking at differences between people in terms of the things that happened to them that we can start to explain mental health issues. Our lecturer says that undoubtedly just from the sheer weight of evidence psychosocial events are the more powerful predictor. We heard about Professor John Read, who believes that the best way to explain the origin of mental health problems - and especially differences between people - is by looking at life events and the different experiences we have in our lives. To get things started we are presented with an article from The British Journal of Psychiatry within which Pat Bracken and colleagues set out an argument for a more social psychiatry; arguing that social factors are the most important determinants of our mental health. Here is their 2012 paper if you’d like to have a read yourself. They argue “… that psychiatry is in the midst of a crisis. The various solutions proposed would all involve a strengthening of psychiatry’s identity as essentially ‘applied neuroscience’. Although not discounting the importance of the brain sciences and psychopharmacology, we argue that psychiatry needs to move beyond the dominance of the current, technological paradigm. This would be more in keeping with the evidence about how positive outcomes are achieved and could also serve to foster more meaningful collaboration with the growing service user movement…”. They says that: ”… Although mental health problems undoubtedly have a biological dimension, in their very nature they reach beyond the brain to involve social, cultural and psychological dimensions. These cannot always be grasped through the epistemology of biomedicine. The mental life of humans is discursive in nature. … The evidence base is telling us that we need a radical shift in our understanding of what is at the heart (and perhaps soul) of mental health practice. If we are to operate in an evidence-based manner, and work collaboratively with all sections of the service user movement, we need a psychiatry that is intellectually and ethically adequate to deal with the sort of problems that present to it. As well as the addition of more social science and humanities to the curriculum of our trainees we need to develop a different sensibility towards mental illness itself and a different understanding of our role as doctors…”. Next we looked at a paper recently published in the journal ‘Schizophrenia Bulletin’ by Filippo Varese and colleagues that I found very interesting as a Children’s Social Worker. Filippo and colleagues explored the link between traumatic childhood experiences (poverty, abuse, etc) and later psychotic experiences. We are told that their work was important because many people tend to think that such serious problems as hallucinations and delusional beliefs are quintessentially biological in origin, and this paper suggests an important social dimension. They looked at a wide range of studies that examined the links between life events and later psychosis. Their conclusions were: ”…Evidence suggests that adverse experiences in childhood are associated with psychosis. To examine the association between childhood adversity and trauma (sexual abuse, physical abuse, emotional/psychological abuse, neglect, parental death, and bullying) and psychosis outcome … we included 18 case-control studies… 10 prospective and quasi-prospective studies… and 8 population-based cross-sectional studies... There were significant associations between adversity and psychosis across all research designs …. patients with psychosis were 2.72 times more likely to have been exposed to childhood adversity than controls. The association between childhood adversity and psychosis was also significant ... These findings indicate that childhood adversity is strongly associated with increased risk for psychosis…” We are directed to read a paper by Ben Barr and colleagues which looked at how the recent economic recession impacted on suicide rates - a rather dramatic (and sad) example of how social factors impact on our mental health. They found that between 2008 and 2010, there were 846 more suicides among men than would have been expected based on historical trends, and 155 more suicides among women. Next we look at a paper in ‘The Psychologist’ by John Read which expresses some frustration at how attempts to integrate biological, social and psychological perspectives on mental health problems tend tacitly to assume that the most important elements are biological, with the social and psychological elements somewhat downplayed. Read argues that people pay lip-service to the bio-psychosocial model, but undermine it in practice. He gives the example of a senior colleague who: ”…acknowledged some of the recent research about the role of psychosocial factors influencing schizophrenia. He concluded, however, that ‘the schizophrenia wars were over years ago’. He was referring to the truce established under the banner of the ‘bio-psycho-social’ model, which says that schizophrenia is an interaction between a genetically inherited predisposition and the triggering effect of social stressors…” He concludes: ”…The simple truths are that human misery is largely inflicted by other people and that the solutions are best based on human – rather than chemical or electrical – interventions…”. Reading this article I can’t help but remember the men I worked with at a service for ex-offenders with drug misuse issues. Most had a dual diagnosis, a number of them schizophrenia, and all had experienced some form of trauma in their childhood or youth. Each of them received medication to treat the condition but “human intervention” was patchy. Our lecturer tells us that we know following 20, 30 years of research that there is no specific genetic predisposition to any of the mental health disorders. And we know that the best predictors by far of all of them, whether it's depression, suicidality, psychosis, are all life events. The strongest predictor all by itself is poverty. Not because poverty by itself causes depression, but because it is a predictor of all the other things that are causal. So poverty has been described as the cause of the causes. And those other causes are a whole raft of things - childhood neglect, childhood abuse, loneliness, and problematic parenting, which is usually inter-generational. It's not about bad parents, it's about parents who themselves haven't perhaps had the sort of childhood that predisposed them to good enough parenting. This is why preventative services, family support and intervention are so vital. Parents need to be taught and supported to break this cycle; and so that children can be safeguarded in the care of their family. This week’s session has left me with little doubt that I favour the social model (this probably won’t come as a surprise to you as I am a Social Worker and Sociology graduate). I hope that following today’s general election we see a greater investment in mental health services as promised in so many of the parties manifestos. I also hope that the next government values children’s social care enough to invest in it and address the woefully inadequate funding for preventative / support services in this country. Spending cuts and austerity have most definitely fallen hardest on the most vulnerable. Have a great week and don’t forget to follow me on facebook so you don’t miss next week’s post on psychology and mental health.  Last week I posted about a course I started entitled Psychology and Mental Health: Beyond Nature and Nurture. Last week's class provided a general introduction to the subject matter and what we should expect from the course over the next few weeks. I was keen to get started.
This week we discussed the role of biological factors - nature - in the development of mental health problems. We heard from Professor John Quinn, who outlined some ways in which neurotransmitter activity affects our moods, and is itself affected by events. We looked at Eric Kandel's 'new intellectual framework for psychiatry'. Eric Kandel is a Nobel prize winning neuroscientist. In addition to his work on memory, Kandel was the author of a very influential and important paper setting out a robust biological account of psychiatry. He argues that all human behaviour, thought and emotion has its roots in the functioning of the brain. Consequently it is to brain-based, neuroscientific, explanations that we should look to for solutions to mental health problems. Kandel argues, in the abstract of his paper, that: ”…In an attempt to place psychiatric thinking and the training of future psychiatrists more centrally into the context of modern biology, the author outlines the beginnings of a new intellectual framework for psychiatry that derives from current biological thinking about the relationship of mind to brain. The purpose of this framework is twofold. First, it is designed to emphasize that the professional requirements for future psychiatrists will demand a greater knowledge of the structure and functioning of the brain than is currently available in most training programs. Second, it is designed to illustrate that the unique domain which psychiatry occupies within academic medicine, the analysis of the interaction between social and biological determinants of behavior, can best be studied by also having a full understanding of the biological components of behaviour…” Kandel then sets out five principles that he believes should provide the underpinnings of a ‘new intellectual framework for psychiatry’. “This framework can be summarized in five principles that constitute, in simplified form, the current thinking of biologists about the relationship of mind to brain.” These are: “Principle 1. All mental processes, even the most complex psychological processes, derive from operations of the brain. The central tenet of this view is that what we commonly call mind is a range of functions carried out by the brain. The actions of the brain underlie not only relatively simple motor behaviors, such as walking and eating, but all of the complex cognitive actions, conscious and unconscious, that we associate with specifically human behavior, such as thinking, speaking, and creating works of literature, music, and art. As a corollary, behavioral disorders that characterize psychiatric illness are disturbances of brain function, even in those cases where the causes of the disturbances are clearly environmental in origin.” “Principle 2. Genes and their protein products are important determinants of the pattern of interconnections between neurons in the brain and the details of their functioning. Genes, and specifically combinations of genes, therefore exert a significant control over behavior. As a corollary, one component contributing to the development of major mental illnesses is genetic.” “Principle 3. Altered genes do not, by themselves, explain all of the variance of a given major mental illness. Social or developmental factors also contribute very importantly. Just as combinations of genes contribute to behavior, including social behavior, so can behavior and social factors exert actions on the brain by feeding back upon it to modify the expression of genes and thus the function of nerve cells. Learning, including learning that results in dysfunctional behavior, produces alterations in gene expression. Thus all of “nurture” is ultimately expressed as “nature.”” “Principle 4. Alterations in gene expression induced by learning give rise to changes in patterns of neuronal connections. These changes not only contribute to the biological basis of individuality but presumably are responsible for initiating and maintaining abnormalities of behavior that are induced by social contingencies.” “Principle 5. Insofar as psychotherapy or counseling is effective and produces long-term changes in behavior, it presumably does so through learning, by producing changes in gene expression that alter the strength of synaptic connections and structural changes that alter the anatomical pattern of interconnections between nerve cells of the brain. As the resolution of brain imaging increases, it should eventually permit quantitative evaluation of the outcome of psychotherapy.” Kandel does not deny that social events are important, but he maintains that social events have their impact on people by affecting the brain: “Viewed in this way, all sociology must to some degree be sociobiology; social processes must, at some level, reflect biological functions. … Nevertheless, it is important to appreciate that there are critical biological underpinnings to all social actions.” Not all psychologists and not all psychiatrists agree with his conclusions, but the paper was definitely worth reading. Next we looked at Nick Craddock and colleagues' 'wake up call for British psychiatry'. Nick Craddock and colleagues drew up a manifesto for the future of psychiatry based at least in part on a biological model of mental health. This 2008 paper was entitled a “Wake-up call for British psychiatry”, and was written by a group of influential and senior psychiatrists. It sets out how a biological model of mental health - the idea that our mental health is determined by our biology - can influence how we design services. Nick and colleagues, in the summary to their paper, argue that: “The recent drive within the UK National Health Service to improve psychosocial care for people with mental illness is both understandable and welcome: evidence-based psychological and social interventions are extremely important in managing psychiatric illness. Nevertheless, the accompanying downgrading of medical aspects of care has resulted in services that often are better suited to offering non-specific psychosocial support, rather than thorough, broad-based diagnostic assessment leading to specific treatments to optimise well-being and functioning. In part, these changes have been politically driven, but they could not have occurred without the collusion, or at least the acquiescence, of psychiatrists. This creeping devaluation of medicine disadvantages patients and is very damaging to both the standing and the understanding of psychiatry in the minds of the public, fellow professionals and the medical students who will be responsible for the specialty’s future. On the 200th birthday of psychiatry, it is fitting to reconsider the specialty’s core values and renew efforts to use psychiatric skills for the maximum benefit of patients”. They begin by arguing that: “… British psychiatry faces an identity crisis. A major contributory factor has been the recent trend to downgrade the importance of the core aspects of medical care”. They argue that this has led to problems: “… In many instances, this has resulted in services that are better suited to delivering nonspecific, psychosocial support rather than a process of thorough, broad-based diagnostic assessment with formulation of aetiology, diagnosis and prognosis followed by specific treatments aimed at recovery with maintenance of functioning…”. and state that: “…Our contention is that this creeping devaluation of medicine is damaging our ability to deliver excellent psychiatric care. It is imperative that we specify clearly the key role of psychiatrists in the management of people with mental illnesses…” Later on, they suggest that: “…In order to follow clinical guidance (such as that provided by the National Institute for Health and Clinical Excellence (NICE)) to develop excellent ‘mental health’ care (for those with mental illness), it is important to recognise that a biomedical component, with access to appropriate facilities and appropriate service pathways, is usually crucial…”. For Nick and colleagues, this is an optimistic vision: “…Major advances in molecular biology and neuroscience over recent years have provided psychiatry with powerful tools that help to delineate the biological systems involved in psychopathology and impairments suffered by patients. We can be optimistic that over the coming years these advances will facilitate the development of diagnostic approaches with improved biological validity and enhanced clinical utility in terms of predicting treatment response. We can expect that completely novel treatments will be developed based on detailed understanding of pathogenesis…”. … “…Psychological and social interventions will, of course, continue to be crucially important in managing psychiatric illness (as they are also in non-psychiatric disorders). However, in addition, patients have the right to expect that biological factors are fully considered and, where appropriate, evidence-based interventions delivered…”. Thirdly, we looked at 'Chemical imbalances'. One powerful idea in the area of mental health is the suggestion that mental health problems result from ‘chemical imbalances’ and that the psychiatric drugs that are commonly prescribed help people because they ‘correct’ these ‘imbalances’. In fact, if you search online for information about mental health problems that is sponsored by pharmaceutical companies, this idea is very common. Dr Joanna Moncrieff is a psychiatrist who has criticised this approach. In essence, her argument is that psychiatric medication has well-recognised effects on the brain, which affect our moods, behaviours and even thoughts, and which can - sometimes - be helpful for people in great distress. But Jo does not support the idea that these drugs are correcting chemical imbalances; and she describes this as the ‘myth of the chemical cure’. Jo advocates that we adopt what she describes as the ‘drug-based’ model of the action of psychiatric medication, rejecting the ‘disease-based’ approach. This does not mean that she believes that the medication is ineffective. She recognises that the medication has a clear effect on our neurotransmitters, and therefore on our emotions and behaviour. But Jo does not believe that this necessarily means that the medication is correcting an underlying abnormality. Finally we concluded with a brief critique of this weeks’ discussions. We are taught that the science and the logical arguments are both strong: we know that the functioning of our brains lies beneath all our behaviours, thoughts and emotions, and so biological approaches cannot be dismissed. And yet, many psychologists and social psychologists think that biological approaches alone cannot fully explain our experience of mental health problems. Next week, we will be looking at social perspectives on mental health. We are challenged, over the course as a whole, to consider how these different approaches can be integrated and to consider the strengths and weaknesses of the biological component of the ‘biopsychosocial model’. I’ll see you again next week…  Cafcass have just published their third survey of Guardians’ views regarding care applications (s31 Children Act 1989) made by local authorities.
The aim was to gauge the views of Guardians in relation to care applications received by Cafcass during the period 11 – 29 November 2013, specifically in relation to:
Key findings from the research include:
This research will come as welcome affirmation to Social Workers in the sector whom seldom see their dedicated work with children and families recognised in the public arena. However, it is disappointing that I was unable to find one news article related to the report during a quick Google search. News agencies are quick to pick up on damning findings from serious case reviews but are not so interested to learn that on the whole Social Workers do a very good job safeguarding and protecting vulnerable children. If you would like to read the research in full you can find it here. |
